Immunotherapy of Advanced Cancers
Unfortunately majority of the cancer patients are diagnosed in late stages, when there are distinct clinical symptoms. By this time in most of the cases there are already visible or invisible metastatic growths which are the main causes for unsuccessful cancer treatment results – causes for relapses, uncontrollable tumor spreads and the causes for short life expectancy. Even in those patients in whom the cancers are found little earlier, by the time they go through the standard harsh scheme of the traditional cancer treatments and realize that these methods are no longer effective, the cancers already outgrow to advance stages.
This is why over last decades, NCI and other cancer institutions are looking for new methods, which could solve these problems. Among others the immunotherapy, mainly in the form of cancer vaccines have been distinguished in this task, achieving many promising results in the cancer world. The only thing is the time factor – it takes minimum 10-15 years before any new medicine could be formulated in the common pharmaceutical market as the standard therapy.
The anticancer vaccine RESAN can be used to treat the advanced cancers, mobilizing its anticancer immunotherapeutical potentials. For this we have elaborated two main approaches utilizing the latest immunotherapeutical techniques: extracorporal activation of anticancer immunocompetent cells (EAAIC) and a complex cancer therapy.

A Complex Cancer Therapy
The development of cancers indicates a failure (due to various reasons) in the complex network of immunological defense system which is present in every organism. This is why a correct complex immunotherapy could have considerable positive effects in the treatment of malignant tumors, which may improve considerably the life expectancy and in certain cases even achieve a complete cure. This can make a great sense especially if the tumor has grown up to 3 and 4 stages.
The complex therapy includes:
1. The maximum resection of the primary tumor and the visible metastases.
2. Use of antitumor vaccine RESAN.
3. Use of cytokines and immunostimulators (IL-1α, IL-2, IFN-γ).
4. Use of thyroid hormones (L-thyroxine).
5. Prevention and treatments of cachexy.
The maximum resection of tumors
When the immune system is matched against a large number of tumor cells, it is more likely to be overwhelmed like an outnumbered army which is one of the main causes for the vaccine to be ineffective during cancer treatment. On the other hand, when the immune system has to detect and fight a smaller number of cancerous cells, it is more likely to be successful in curing cancers, for example when the tumors have not grown too large sizes or when the primary tumor has been eliminated by surgery. This is why better results are obtained when we resect out the primary tumor and the visible metastases as maximum as possible.
Use of antitumor vaccine RESAN
The most optimum time to inject the vaccine is 7-12 days prior the operation, though good results are obtained when it is injected 7-14 days after the operation too. However, if the vaccine has been missed to inject with in this period, it can be injected later too, but it is important to note that earlier it is injected the better the result you get.
Use of citokines and immunostimulators
Similarly, the use of cytokines has shown a considerable significance in the complex immunotherapy. The doses and the number of injections of cytokines needed to administer depend on the immune status and the moment at which the vaccine is administered.
Interleukin-1α (IL-1α ) helps to restore the weakening antitumoral immunity, decelerates the tumor growth and reduces its' metastatic potential. IL-1α should be injected prior to the vaccine administration if CD4 > 350 and CD8 < 280 in order to re-establish the immune system. IL-1α, in such case, should be injected 5 days continuously through i. v. drip-feed, within 30-40 minutes at the dose of 15 ng per kg mass.
The changes of the immune status after a course of IL-1α
The vaccine is applied after getting the better parameters of the immun status. After the injection of vaccines, a back-up immunotherapy with IL-1a is applied for 6-12 months. The back-up course is prescribed once in two months which includes: 2 injections daily at the dose of 15 ng per kg mass, even in the case when CD4 > 350 and CD8 > 280. If the number of lymphocytes has decreased lower the given margin (CD4 < 350, CD8 < 280) a full course of IL-1a is prescribed.
Interleukin 2 (IL-2) is used on 10-14 days after the injection of vaccines at the dose of 100000-125000 IU per m2 surface area of the, daily, through i. v. drip feed within 4 hrs. A full course therapy consists of 15-60 of such injections. Further, IL-2 immunotherapy is applied at an interval of 2 months for 6-12 months. A single back-up course of IL-2 consists of 125000 IU per m2 daily for 4 days.
Gamma interferon (IFN-γ) is used according to the following scheme: intramuscular injection of 1000000 IU IFN-g on every second day for a month and then once a week for 2 months. Gamma interferon is started to applied from the next day after the RESAN injections.
Better results were observed when IL-2 and IFN-γ could have been supplied directly into the tumors during the basic course of immunotherapy.
It is compulsory to use L-thyroxine during the complex immunotherapy. L-thyroxine is prescribed as 25 mcg (microgram), under tongue everyday in the morning for 4-6 months. Then, it is withdrawn slowly reducing 25 mcg (microgram) every week.
Prevention and treatments of cachexy
During the cancer patient care it is important to have regular weight checkings (once in 2 months), as in 50-80 % of the patients with advancing cancer growths develops cachexia. Cachexia is said to be developed when the patients lose more than 5 % of premorbidal weight within six months period. Cachexia - a word from Greek derivation: "kakos" – poor and "hexis" – state. The development of a cachexia in cancer patients indicates a bad prognosis and a considerable decline in the patient's general health condition. In fact cachexia is the principal cause of deaths among the cancer patients. The main mechanism is the hypermetabolism that takes place in most of the cancer patients. The major clinical signs of the hypermetabolism are fatigue, apathy and depression. As a whole it affects the protein, fat and carbohydrate metabolisms.
For the prevention and treatments of cachexy the following therapy is recommended:
1. Peritol (Cyproheptadine) 4 mg, 4 times a day, daily, constantly.
2. Dexamethasone 4 mg, once a day, daily for one week.
Dexamethasone is better to take in the morning during breakfast. If the appetite of the patient increases then dexamethasone is taken constantly; where as if there is no changes in appetite then dexamethasone is replaced by medroxyprogesterone at the doses - 500 mg, 2 times a day. If medroxyprogesterone is not found, it can be replaced by megestrol acetate at the doses - 40 mg, 4 times a day.
If the necessary effects are not achieved then the doses of megestrol acetate is increased gradually first 80 mg, 4 times a day then 100 mg 4 times a day. If you still don't get the effect, then megestrol acetate is prescribed as 200 mg, 4 times a day.
3. Ibuprofen at a dose of 400 mg, three times, daily OR indomethacin at a dose of 50 mg twice a daily.
4. Almagel, 1 tea spoon, 20-30 minutes before the intake of ibuprofen or indomethacin.
5. Activated carbon, 2 g at night, daily.
6. Fish-oil, 1 tea spoon, once a week.
Resan vaccine which can release intensive pain symptoms
Beside the anticancer specific immune responses, RESAN increases the number and functional activeness of the natural killers – CD56 lymphocytes, which secrete beta-endorphins in large amounts. In our body beta-endorphins are responsible to block out the pain signals. So more the amount of these substances in our body the higher the pain threshold.
Due to this, the vaccine administration may release the pain symptoms (in fact one of the dominant clinical problems in the late stage cancer patients) considerably. This would in turn, improve the general life-style of the cancer patients.
Extracorporal Activation of Anticancer Immune-competent Cells (EAAIC)
The vaccine RESAN can be used in an extra corporal (outside the organism) activation of immunocompetent blood cells of cancer patient, specifically sensitive to response against cancer antigens, which are in turn are returned back to the patient to destroy cancer cells.
As a result of leucocyte activation, it is possible to derive autogenous cytokines of an early phase of the immune answer for a particular patient which then, can be returned back in optimal, physiologically balanced proportions. Because of the fact that these cytokines are of own, antibodies against them do not form, in difference to that when used recombinant cytokines. This enables to maintain the activity of autogenous cytokines constantly in a high level increasing the overall efficiency of the applied immunotherapy.
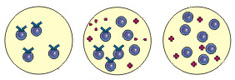
The production of the cytokines of an early phase of the immune answer
Fig. 1
Utilizing a vaccine in extracorporal activations of lymphocytes we can select a particular clone of lymphocytes activated against a particular tumor of the patient as well. Then, having multiplied these highly activated lymphocytes we return them back into the patient which significantly increases the antitumoral immune answer.
Both of these methods can be used together or separately. The only thing is that they can be conducted only in clinics equipped by special equipments for separation of blood cells and cell culture.
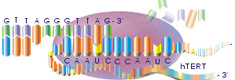
The production of the antitumoral T-lymphocytes

Fig. 2